Adding biomarker evidence to your existing algorithm may help increase your confidence in diagnosing Alzheimer’s disease (AD)1-6
Blood-based biomarkers could play a key role in identifying individuals who should be referred to specialists for further evaluation, which may include PET imaging or CSF analysis7
Blood tests are currently used to identify the probability of the presence or absence of amyloid plaques in the brain8
Phosphorylated tau, or P-tau, is a key blood-based biomarker for AD, and P-tau217 is considered the most reliable blood-based biomarker in helping to detect evidence of AD pathology, including amyloid9,10
In conjunction with clinical assessment, P-tau217 has a strong correlation with amyloid PET scans, making it a valuable blood-based biomarker for detecting AD pathology, including amyloid, in its initial stages9,10
Patients must meet testing criteria. These tests are not intended to be used as a standalone diagnostic; they must be utilized with other clinical assessment results.
In conjunction with clinical assessments, blood-based biomarker tests can be used to detect or rule out evidence of AD pathology, including amyloid, primarily for patients aged ≥65 years, given their higher rate of amyloid positivity. Younger patients who meet the test’s intended use may also be considered.10,11
PET scans and CSF tests are also available to help assess amyloid pathology in patients with suspected AD, and there are additional AD biomarkers beyond P-tau217 that could be considered in a diagnostic workup.10
Many blood tests* that include P-tau217 can be highly accurate for confirming or ruling out AD pathology, including amyloid, in patients with cognitive decline or MCI12
A head-to-head study† of leading blood-based biomarker assays for AD identified plasma P-tau217 as the most accurate for detecting AD pathology. The study also showed %P-tau217‡ had a slightly stronger correlation with amyloid PET than P-tau assays alone.13§
In another study with primary care physicians, %P-tau217 improved diagnostic accuracy for AD pathology from 58% with standard clinical evaluation to 90% when combined with clinical assessment.14||
P-tau217 Ratio (%P-tau217) Demonstrates Clinical Utility in Diagnosing AD14||
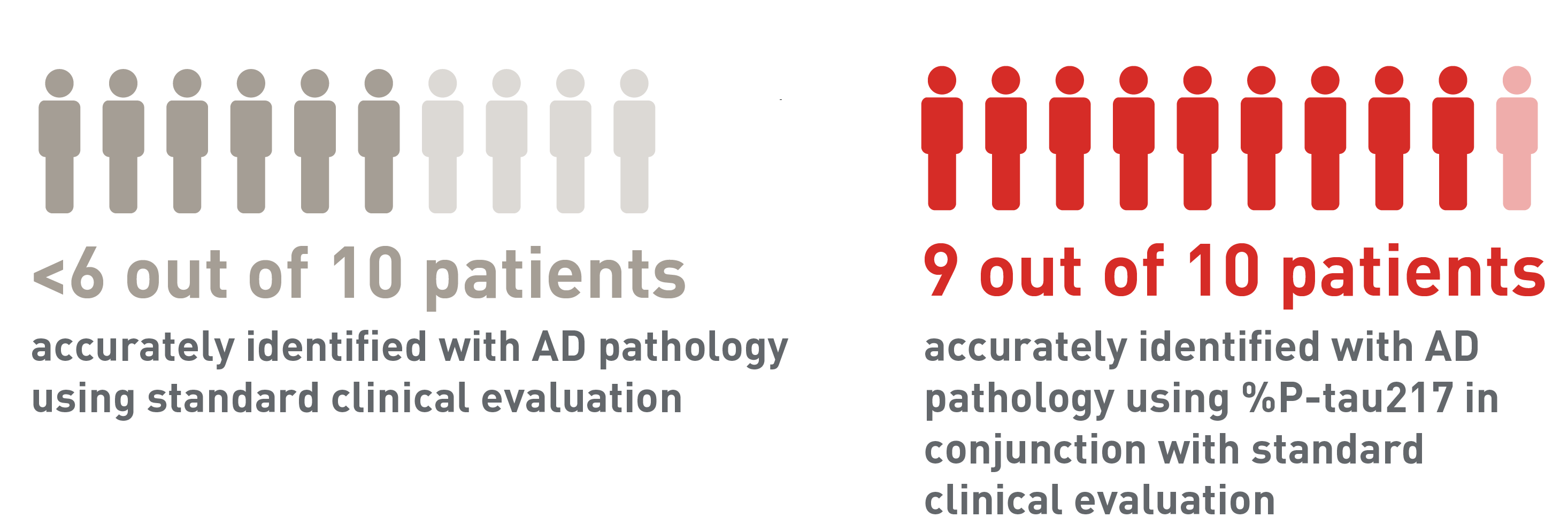
Visuals comparing the diagnostic accuracy of standard clinical evaluation and %P-tau217 in conjunction with standard clinical evaluation. Less than 6 out of 10 patients were accurately identified with AD pathology using standard clinical evaluation. 9 out of 10 patients were accurately identified with AD pathology using %P-tau217.
Commercially available P-tau217 blood tests are not standalone tests. The results must be utilized with clinical assessment results.10
PET scans and CSF tests are also available to help assess amyloid pathology in patients with suspected AD, and there are additional AD biomarkers beyond P-tau217 that could be considered in a diagnostic workup.10
Commercially available P-tau217 assays in the United States15-24¶
Company
Neurocode
Test Name
ALZpath Dx: Plasma
Phosphorylated Tau 217 [P-tau217]
Company
Quest Diagnostics
Test Name
AD-Detect™ ABeta 42/40 and p-tau217 Evaluation
Company
Quest Diagnostics
Test Name
Quest AD-Detect© Phosphorylated tau217 [P-tau217]
This list only includes some commercially available tests. It is only intended for informational purposes and your consideration, and is based on publicly available information as of June 30, 2025. Eli Lilly and Company (Lilly) makes no representations regarding the clinical or analytical validity, manufacturing quality, or design of the testing offered by the vendors included on this list. Inclusion on this list does not represent an endorsement, referral, or recommendation by Lilly nor representation of assay performance compared to CEOi** acceptable performance criteria for a confirmatory or triage assay. Contact the laboratory vendor for more information. All other trademarks are property of their respective owners.
Commercially available P-tau217 blood tests are not standalone tests. The results must be interpreted in conjunction with clinical assessment results.10
Integrating blood biomarker tests into your clinical assessment
- Collect a blood sample according to the processing instructions provided by the performing laboratory. Be sure to closely adhere to these instructions
- Follow the performing laboratory’s guidance on how to store and ship the specimen to the testing lab for analysis
Thought Leader (TL) Consensus** recommends selecting a blood test that has ≥90% sensitivity, ≥85% specificity, and <20% intermediate results for use as a triage test.10††
For triage assays that meet consensus performance criteria:
Result Concordance With Amyloid PET
|
Recommended Next Steps
|
|---|---|
| Result Concordance With Amyloid PET Positive | Recommended Next Steps Refer to specialist |
| Result Concordance With Amyloid PET Intermediate | Recommended Next Steps Refer to specialist |
| Result Concordance With Amyloid PET Negative | Recommended Next Steps Further assessment needed |
Table presenting the Thought Leader (TL) Consensus guidance for interpreting blood tests—assays meeting performance criteria for triage assay: If the result concordance with amyloid positron emission tomography (PET) is positive: along with full clinical assessment, supports the increased likelihood of having Alzheimer’s disease (AD) pathology, including amyloid. Recommended next step: refer to a specialist for further evaluation and additional workup. If the result concordance with amyloid PET is intermediate: does not provide a clear answer regarding the status of AD pathology, including amyloid. Recommended next step: consider referral to a specialist for further evaluation and additional workup, which may involve repeating the blood test. If the result concordance with amyloid PET is negative: strongly supports the absence of AD pathology, including amyloid. Recommended next step: further assessment is needed. Consider further assessment for causes of cognitive impairment other than AD.
PET scans and CSF tests are also available to help assess patients with suspected AD.10
Hear from a neurology expert on the importance of a complete workup prior to referral
VO: Dr Galvin was paid for his time and participation.
Dr Galvin:
[Introduction]
Hello, I’m Dr James Galvin, and I’m a Cognitive Neurologist. I’ve been practicing for 30 years and am board-certified in Neurology.
[Patient background]
Today, I’d like to share a case that illustrates how I confirm a diagnosis of early-stage Alzheimer’s disease and how primary care providers and neurologists can partner to refer appropriate patients.
Nancy, a 70-year-old retired high school teacher, came to see me with her husband, Bill. Nancy was mostly independent in her daily activities but recently developed mild memory loss and irritability. She was having trouble remembering scheduled events and frequently misplaced items like her keys. Maintaining her independence is incredibly important to both Nancy and Bill.
[Diagnosis]
My first step was to understand what Nancy was experiencing, her family history, and previous major health issues. I conducted a comprehensive evaluation, including a medication review. I administered a patient interview and a mood assessment to rule out depression, as well as the MoCA. Nancy’s result was suggestive of cognitive deficit with a MoCA score of 24.
I then ordered a brain MRI to investigate potential causes of cognitive impairment and look for any lesions. There was mild cortical and hippocampal atrophy with no evidence of stroke, microhemorrhages, or mass lesions. This pattern on the MRI was supportive of Alzheimer’s disease as the most likely cause.
EFFICACY/SAFETY DISCLAIMERS ON SCREEN DURING THE BELOW PARAGRAPH
I decided to perform a blood-based biomarker evaluation to help identify Alzheimer’s pathology. There are several blood-based biomarker tests available, such as Aβ 42/40, P-tau181, and P-tau217. I typically use the P-tau217 blood test for my patients, because it’s highly concordant with amyloid PET.
I discussed blood-based biomarker testing with Nancy and Bill, including the potential risks and benefits, as well as costs and insurance coverage. Nancy consented to the P-tau217 test, and we proceeded.
Her test result was positive based on the blood biomarker results. I wanted to order an additional test to confirm the presence of amyloid.
I typically order an amyloid PET scan for patients who consent and have a positive P-tau217 test. If, for any reason, a PET scan is not an option, I would consider CSF.
In this case, Nancy was open to PET, so we proceeded, and it came back positive. From these PET results, in combination with a MoCA score of 24, MRI results, and a positive P-tau217 test, I was able to confirm Alzheimer’s disease neuropathology and diagnose Nancy with mild cognitive impairment due to Alzheimer’s disease.
In many cases, primary care physicians refer patients with suspected Alzheimer’s to me. It’s incredibly helpful when they’ve already conducted a clinical workup, including cognitive assessment, MRI, and blood-based biomarker testing like P-tau217. P-tau217 can serve as an effective triage tool, allowing PCPs to refer patients with a positive or intermediate result.
This approach saves patients time and streamlines the referral process. When patients are referred with cognitive assessments, blood-based biomarker tests, and MRI results, we can make our first visit more productive and focused.
I can then perform additional confirmatory tests, using the PCP’s testing results as part of the diagnostic process. Most blood tests, including P-tau217, can be conducted in a primary care setting, offering a more accessible and less invasive testing option.
In conjunction with clinical assessments, blood tests that include P-tau217 can support PCPs in making informed decisions about specialist referrals for further evaluation and additional testing.
After confirming Nancy’s diagnosis, I sat down with her and Bill to discuss potential treatment options that are available should she elect to move forward. Nancy decided to move forward with treatment, and she now receives routine care to help manage her condition. Nancy and Bill feel hopeful that they can enjoy more quality time together.
[Conclusion]
Timely assessment of cognitive impairment, followed by blood-based biomarker testing, can enable rapid and appropriate referrals to someone like me. It allows me as a specialist to confirm or rule out Alzheimer’s disease pathology promptly and accurately, and then provide appropriate disease management, which may make a meaningful difference for patients.
For informational purposes only. Not an endorsement of any Lilly product.
PP-AD-US-0833 07/2025 ©Lilly USA, LLC 2025. All rights reserved.
Explore resources to support early AD diagnosis
Additional diagnostic tools
CSF testing1,2
- Determine amyloid beta (eg, CSF Aβ42/Aβ40) and tau protein (eg, total tau and phosphorylated tau) levels measured in cerebrospinal fluid. Learn more about CSF tests
- A multidisciplinary workgroup convened by the Alzheimer’s Association developed appropriate use criteria (AUC) for the use of CSF testing for AD pathology detection in the diagnostic process.25 Explore CSF AUC
Biomarker PET scans4,5,8
- Used to determine presence of abnormal amyloid plaque and aggregated tau NFTs
- Provides the means to assess visual evidence of brain amyloid and tau pathology in vivo
- Approved amyloid PET scans are available for use at your discretion. Learn more about a biomarker PET scan
- The Alzheimer’s Association and the Society of Nuclear Medicine and Molecular Imaging developed AUC for amyloid PET scans.26
- Explore amyloid PET AUC
Earlier consideration of therapeutic options27,28
- Opportunity to consider available therapies approved for AD
- Access to clinical trials with potential to benefit from current and future therapies that address the underlying pathology of the disease and contribute to local research opportunities
Other routine diagnostic tools used in the assessment of patients include:
- Labs: CBC, electrolytes, BUN, Cr, Ca, LFTs, glucose, TSH, B12, folate; consider RPR or MHA-TP (per patient history), HIV, heavy metals27,29,30
- Structure neuroimaging (MRI)27,29,30
- Neuropsychological assessment3,31
- FDG-PET scan3,31
%P-tau217=ratio of P-tau217 to non–P-tau217 (expressed as percentage of P-tau217); Aβ=amyloid beta; BUN=blood urea nitrogen; Ca=calcium; CBC=complete blood count; CEOi=CEO Initiative; Cr=creatinine; CSF=cerebrospinal fluid; CT=computed tomography; FDG-PET=fluorodeoxyglucose-positron emission tomography; HIV=human immunodeficiency virus; LFTs=liver function tests; MCI=mild cognitive impairment; MHA-TP=microhemagglutination assay for Treponema pallidum antibodies; MRI=magnetic resonance imaging; NFTs=neurofibrillary tangles; PET=positron emission tomography; RPR=rapid plasma regain; TSH=thyroid stimulating hormone.
*Must meet testing criteria.
†This study compared the performance of leading plasma biomarkers in detecting AD pathology and guiding treatment and clinical trial inclusion. A total of 1,179 plasma samples from 393 Alzheimer’s Disease Neuroimaging Initiative (ADNI) participants were analyzed using assays from C2N Diagnostics, Fujirebio, ALZpath Quanterix, Janssen LucentAD Quanterix, and Roche NeuroToolKit. Plasma biomarkers P-tau217, P-tau181, and Aβ42/Aβ40 were assessed for their ability to classify amyloid PET status, tau PET status, cortical thickness, and cognitive impairment, with clinical assessments including the Clinical Dementia Rating (CDR).13
‡P-tau217 used as a ratio, calculated as P-tau217 divided by non-phosphorylated tau217.13
§%P-tau217 demonstrated an AUC of up to 0.93, outperforming other P-tau217 assays, which ranged from 0.88 to 0.90.13
||In a study of 1213 patients with cognitive symptoms, blood tests were evaluated for AD pathology. The study used predefined cutoff values to assess the ability of %P-tau217 levels (the ratio of P-tau217/non-phosphorylated-tau217) alone and combined with the Aβ42/Aβ40 ratio as a composite amyloid probability score (APS2) to identify AD pathology. Blood samples from both primary and secondary care groups were analyzed as a single batch or biweekly, comparing diagnostic accuracy between the blood tests and primary care physicians or dementia specialists. Secondary objectives included examining biomarker performance at various cognitive stages and testing different cutoff values.14
¶This list includes most LDTs for use in the United States and may not be available in all states due to state licensure requirements. This list includes tests that have no care setting specified or are intended for use in the primary care setting. LDTs are diagnostic tests that are designed, manufactured, and used in a single laboratory. The Food and Drug Administration (FDA) can approve or clear IVD tests, but the LDTs included here have not been evaluated, approved, or cleared by the FDA. Only certain labs are certified under Clinical Laboratory Improvement Amendments (CLIA) as qualified to perform high-complexity clinical testing.
**The Global CEOi BBM Workgroup is a partnership consisting of individuals in academia who help validate blood-based biomarker tests and diagnostics, the medical device companies that develop them, pharmaceutical companies developing treatment pathways where BBMs may be useful, and patient advocacy groups that aim to improve AD care and treatment. Together, CEOi works to address major challenges in the field of AD and the BBM workgroup was established to examine the minimum acceptable performance standards of BBM tests in clinical use. Their recommendations are based on an assay’s validation performance data, and real-world results may vary depending on clinical setting.10
††Patients must meet testing criteria.
References:
- McDade E, Bednar M, Brashear HR, et al. The pathway to secondary prevention of Alzheimer’s disease. Alzheimers Dement (N Y). 2020;6(1):e12069. doi:10.1002/trc2.12069
- Aisen PS, Cummings J, Jack CR Jr, et al. On the path to 2025: understanding the Alzheimer’s disease continuum. Alzheimers Res Ther. 2017;9(1):60. doi:10.1186/s13195-017-0283-5
- Hort J, O’Brien JT, Gainotti G, et al. EFNS guidelines for the diagnosis and management of Alzheimer’s disease. Eur J Neurol. 2010;17(10):1236-1248. doi:10.1111/j.1468-1331.2010.03040.x
- Grundman M, Pontecorvo MJ, Salloway SP, et al. Potential impact of amyloid imaging on diagnosis and intended management in patients with progressive cognitive decline. Alzheimer Dis Assoc Disord. 2013;27(1):4-15. doi:10.1097/WAD.0b013e318279d02a
- Counts SE, Ikonomovic MD, Mercado N, et al. Biomarkers for the early detection and progression of Alzheimer’s disease. Neurotherapeutics. 2017;14(1):35-53. doi:10.1007/s13311-016-0481-z
- McKhann GM, Knopman DS, Chertkow H, et al. The diagnosis of dementia due to Alzheimer’s disease: recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimers Dement. 2011;7(3):263-269. doi:10.1016/j.jalz.2011.03.005
- Hampel H, O’Bryant SE, Molinuevo JL, et al. Blood-based biomarkers for Alzheimer’s disease: mapping the road to the clinic. Nat Rev Neurol. 2018;14(11):639-652. doi:10.1038/s41582-018-0079-7
- Iaccarino L, Burnham SC, Dell’Agnello G, et al. Diagnostic biomarkers of amyloid and tau pathology in Alzheimer’s disease: an overview of tests for clinical practice in the United States and Europe. J Prev Alzheimers Dis. 2023;10(3):426-442. doi:10.14283/jpad.2023.43
- Ashton NJ, Brum WS, Di Molfetta G, et al. Diagnostic accuracy of a plasma phosphorylated tau 217 immunoassay for Alzheimer disease pathology. JAMA Neurol. 2024;81(3):255-263. doi:10.1001/jamaneurol.2023.5319
- Schindler SE, Galasko D, Pereira AC, et al. Acceptable performance of blood biomarker tests of amyloid pathology — recommendations from the Global CEO Initiative on Alzheimer’s Disease. Nat Rev Neurol. 2024;20(7):426-439. doi:10.1038/s41582-024-00977-5
- Mielke MM, Anderson M, Ashford JW, et al. Recommendations for clinical implementation of blood-based biomarkers for Alzheimer’s disease. Alzheimers Dement. Published online October 1, 2024. doi:10.1002/alz.14184
- Hansson O, Edelmayer RM, Boxer AL, et al. The Alzheimer’s Association appropriate use recommendations for blood biomarkers in Alzheimer’s disease. Alzheimers Dement. 2022;18(12):2669-2686. doi:10.1002/alz.12756
- Schindler SE, Petersen KK, Saef B, et al; Alzheimer’s Disease Neuroimaging Initiative (ADNI) Foundation for the National Institutes of Health (FNIH) Biomarkers Consortium Plasma Aβ and Phosphorylated Tau as Predictors of Amyloid and Tau Positivity in Alzheimer’s Disease Project Team. Head-to-head comparison of leading blood tests for Alzheimer’s disease pathology. Alzheimers Dement. 2024;20(11):8074-8096. doi:10.1002/alz.14315
- Palmqvist S, Tideman P, Mattsson-Carlgren N, et al. Blood biomarkers to detect Alzheimer disease in primary care and secondary care. JAMA. 2024;332(15):1245-1257. doi:10.1001/jama.2024.13855
- ARUP® Laboratories. Lab test directory page. Phospho-tau 217, plasma. Accessed April 29, 2025. https://ltd.aruplab.com/Tests/Pub/3019017
- C2N Diagnostics. PrecivityAD2™. Accessed December 17, 2024. https://precivityad.com/precivityad2-hcp
- Labcorp. Phosphorylated tau 217 (pTau-217), plasma test. Accessed October 29, 2024. https://www.labcorp.com/tests/484390/phosphorylated-tau-217-ptau-217-plasma
- Labcorp. Phosphorylated Tau 217/Beta Amyloid 42 Ratio, Plasma. Labcorp Test Directory. Updated April 10, 2025. Accessed April 29, 2025. https://www.labcorp.com/tests/505415/phosphorylated-tau-217-beta-amyloid-42-ratio-plasma
- Lucent Diagnostics. About LucentAD for providers. Accessed April 29, 2025. https://www.lucentdiagnostics.com/lucentad-p-tau-217/
- Lucent Diagnostics. LucentAD® Complete. Accessed May 22, 2025. https://www.lucentdiagnostics.com/tests/lucentad-complete/
- Mayo Lab. Phosphorylated tau 217 (pTau-217) test overview. Accessed October 29, 2024. https://www.mayocliniclabs.com/test-catalog/Overview/621635
- Neurocode. ALZpath Dx: Plasma Phosphorylated Tau 217 (p-Tau 217). Neurocode Test Directory. Accessed April 29, 2025. https://neurocode.com/test/alzpath-plasma-phosphorylated-tau-217/
- Quest Diagnostics™. Quest AD-Detect® phosphorylated tau 217 (pTau217), plasma. Accessed October 29, 2024. https://testdirectory.questdiagnostics.com/test/test-detail/13825/quest-ad-detect-phosphorylated-tau217ptau217-plasma?p=r&q=ptau&cc=MASTER
- Quest Diagnostics™. AD-Detect™ Aβ42/40 and p-tau217 Evaluation, Plasma. Quest Diagnostics Test Directory. Accessed April 29, 2025. https://testdirectory.questdiagnostics.com/test/test-detail/14258/addetectabeta-4240-and-ptau217-evaluationplasma?q=14258&cc=MASTER
- Shaw LM, Arias J, Blennow K, et al. Appropriate use criteria for lumbar puncture and cerebrospinal fluid testing in the diagnosis of Alzheimer’s disease. Alzheimers Dement. 2018;14(11):1505-1521. doi:10.1016/j.jalz.2018.07.220
- Johnson KA, Minoshima S, Bohnen NI, et al; Alzheimer’s Association. Appropriate use criteria for amyloid PET: a report of the Amyloid Imaging Task Force, the Society of Nuclear Medicine and Molecular Imaging, and the Alzheimer’s Association. Alzheimers Dement. 2013;9(1):e1-e16. doi:10.1016/j.jalz.2013.01.002
- Porsteinsson AP, Isaacson RS, Knox S, et al. Diagnosis of early Alzheimer’s disease: clinical practice in 2021. J Prev Alzheimers Dis. 2021;8:371-386. doi:10.14283/jpad.2021.23
- Galvin JE, Aisen P, Langbaum JB, et al. Early stages of Alzheimer’s disease: evolving the care team for optimal patient management. Front Neurol. 2021;11:592302. doi:10.3389/fneur.2020.592302
- Scharre DW, Trzepacz PT. Evaluation of cognitive impairment in older adults. Focus (Am Psychiatr Publ). 2013;11(4):482-500. doi:10.1176/appi.focus.11.4.482
- Act on Alzheimer’s. Clinical provider practice tool. Revised June 22, 2016. Accessed April 13, 2022. http://www.actonalz.org/sites/default/files/documents/ACT-Provider-ClinicalPracticeTool.pdf
- Albert MS, DeKosky ST, Dickson D, et al. The diagnosis of mild cognitive impairment due to Alzheimer’s disease: recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimers Dement. 2011;7(3):270-279. doi:10.1016/j.jalz.2011.03.008