
Time is of the essence for patients with Alzheimer's disease (AD)1,2
AD diagnosis is delayed on average by 2-3 years after onset of symptoms and is often made only in the later stages of the disease2-4
AD is the most common cause of dementia and a top 10 leading cause of death in the US among individuals 65 years of age and older4,5*
An estimated 7.2 million Americans age 65 and older are living with AD dementia4
≥50% of patients with Alzheimer’s dementia are not diagnosed in the early symptomatic stages of the disease4
As of 2024, nearly 12 million Americans take care of a family member or friend with dementia4
*Based on data from 2022, the most recent year for which final national mortality data is available.4
Timely detection and diagnosis of AD are important because they may enable earlier initiation of informed disease management, earlier opportunities to support cognitive well-being, and earlier consideration of therapeutic options.2,6
Early detection of AD begins with identifying the right patient2,3
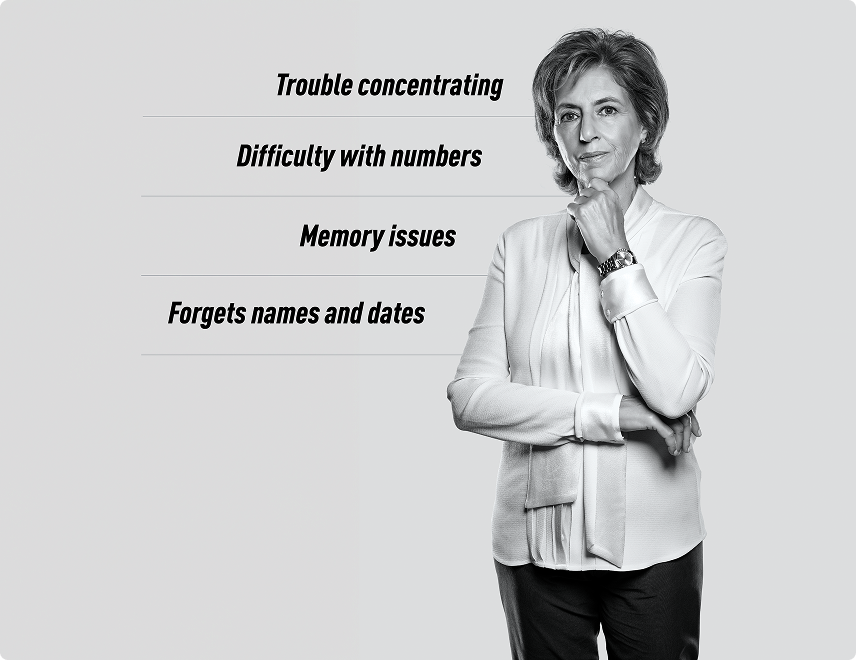
Consider referring patients in your practice for further diagnostic evaluation who:
Display subtle difficulties with memory, language, or thinking, and may downplay or dismiss concerns, such as trouble concentrating, difficulty with numbers, or forgetting names and dates2,7
Continue to maintain independence despite mild cognitive symptoms, and report experiencing little to no impact on daily activities or functional abilities2,7,8
Are strongly motivated to understand the cause of their cognitive decline and are open to treatment
Additional symptoms of early symptomatic AD to watch out for2
Behavioral: social withdrawal, impulsivity
Examples: avoiding social activities, altered judgement
Psychological: depression, mood changes, apathy
Examples: loss of purpose, reduced initiative
Amyloid-targeting therapies (ATTs) are approved for patients with mild cognitive impairment (MCI) and mild dementia, underscoring the importance of referral at the first signs of cognitive impairment2,3,7,9
Defining early symptomatic AD
Characterizations of the AD stages from the National Institute on Aging and The Alzheimer’s Association2,10
AD Continuum2,8-12
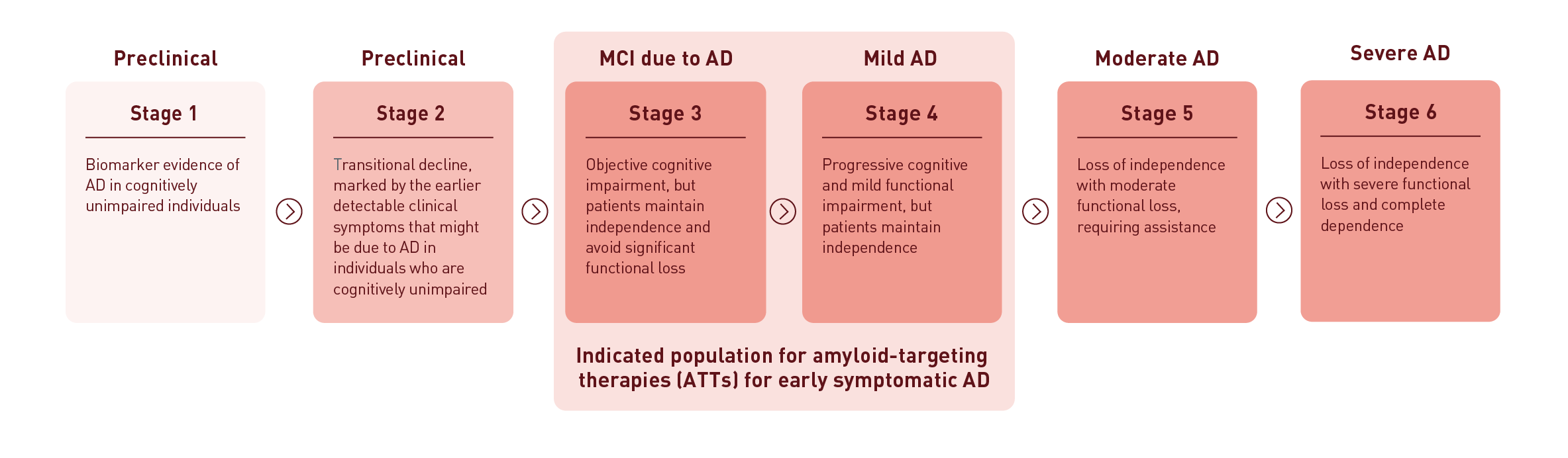
Schematic of the progressive Alzheimer’s disease (AD) continuum, from stage 1 through stage 6. Stage 1 presents as biomarker evidence of AD in cognitively unimpaired individuals. Stage 2 presents as transitional decline, marked by the earlier detectable clinical symptoms that might be due to AD in individuals who are cognitively unimpaired. Stages 3 and 4—the indicated population for amyloid-targeting therapies (ATTs) for early symptomatic AD—include mild cognitive impairment (MCI) due to AD and mild AD, respectively. Stage 3 presents as objective cognitive impairment, but patients maintain independence and avoid significant functional loss. Stage 4 presents as progressive cognitive and mild functional impairment, but patients maintain independence. Stage 5 presents as loss of independence with moderate functional loss, requiring assistance and Stage 6 presents as loss of independence with severe functional loss and complete dependence.
38% of individuals in the US with mild AD are estimated to progress to moderate or severe AD annually13,14†
†This study estimated annual progression rates in amyloid-positive patients across the AD continuum, leveraging longitudinal prospective data from the US National Alzheimer’s Coordinating Center (NACC) Uniform Data Set. This data set included nearly 30,000 patients with varying levels of cognitive impairment collected from September 2005 through December 2017 from approximately 30 Alzheimer’s disease research centers across the US. Patients in the prevalent population (n=4370) had a mean age of 77.72 (standard deviation [SD]: 10.48). Females comprised 51.0% of the population. The breakdown of Clinical Dementia Rating Health State was: 2.9% asymptomatic, 9.3% MCI-AD, 11.9% Mild AD Dementia, 21.5% Moderate AD Dementia, 30.6% Severe AD Dementia, and 23.8% died. Some patients progressed by more than one stage in 1 year (e.g., MCI-AD to moderate or severe AD dementia).13
Key limitations of this study included the fact that NACC data are not precisely 1 year. In addition, amyloid-positive patients represented a small subset of the overall NACC patient sample, and therefore may not be generalizable. Based on this, the authors collaborated with clinical experts to develop an approach of identifying amyloid-positive patients. Patients were considered amyloid positive if, within 10 years of their first visit, they had either 1) abnormally elevated amyloid on a PET scan, 2) abnormally low amyloid based on CSF, or 3) autopsy result consistent with a patient having been amyloid positive.13
The above data/information is obtained from real-world evidence (RWE) studies. Real-world evidence differs from evidence derived from clinical trials in terms of study design and methodology, patient population, the way in which treatments are assigned (random vs non-random), outcomes assessed, and source of data. Results from RWE are not intended for direct comparison to clinical trial results and should be viewed as complementary information.
In AD, changes in the brain can begin years before symptoms appear1,15
Up to 20 years before the clinical symptoms of AD emerge, pathophysiological changes are thought to take place—including the abnormal buildup of amyloid plaques and hyperphosphorylated tau.2
Significant neurodegeneration: by the time clinical symptoms emerge1,16-18
Synaptic loss and neuronal death may result from the abnormal accumulation of amyloid and tau, ultimately leading to clinical symptoms of cognitive impairment and eventually dementia.1,16-18
00:03
[Main Title Screen]
Caption: Hallmark Biomarkers of Alzheimer’s Disease
[Lilly promotional code line and logo at bottom]
Caption: PP-AD-US-0294 3/2022 © Lilly USA, LLC 2022. All rights reserved.
00:07
[Begin with outline of person, highlight brain and bring rotating brain to the foreground.]
Narrator: Alzheimer’s disease is a progressive brain disorder that causes a gradual and irreversible loss of higher brain functions, leading to dementia and eventually death due to the debility associated with this disease.1,2
00:18
[Window-out key images – Titled visuals of: amyloid plaque, neurofibrillary tangles, and neuronal death.]
Caption: Amyloid Plaque
Caption: Neurofibrillary Tangles
Caption: Neuronal Death
Narrator: Pathologic hallmarks of Alzheimer’s disease include amyloid plaques, neurofibrillary tangles, and degeneration and loss of neurons and their synapses.1,3,4
00:33
Narrator: The development of biomarkers has helped to clarify the likely sequence of events that occurs in people with Alzheimer’s disease.5,6
00:41
[Animated visuals of different a-beta peptide formations, tau, and NFTs]
Narrator: While there are many unanswered questions, the prevailing theory suggests that abnormal production and clearance of the peptide in the brain called amyloid beta, or A-beta, initiates a complex series of pathological and toxic events.5,6
00:58
[Cliff Jack Figure – first visual includes only the a-beta line on graph along with axes labeling]
Caption
Clinical disease stage
Biomarker magnitude
Abnormal
Normal
Cognitively normal
MCI
Dementia
Narrator: A series of pathological events occur at different stages of the disease, as shown here in this prominent model of Alzheimer’s disease.7
This sequence of events is expressed as a hypothetical model of Alzheimer’s disease that describes a decades-long process beginning with the accumulation of A-beta in the brain,7
01:17
[Cliff Jack Figure – includes both a-beta and tau lines]
Narrator: …followed by the development of tau pathology,7
01:20
[Cliff Jack Figure – includes the 1) a-beta, 2) tau, 3) brain structure lines on graph]
Narrator: … synaptic dysfunction and neuronal death.7
01:24
[Cliff Jack Figure – includes the 1) a-beta, 2) tau, and 3) brain structure,4) memory and 5) clinical function lines on graph
- Animated entry of oblong circle appears around Med/Clin Fxn lines
- Next – a-beta line is circled]
Narrator: By the time that even subtle signs of dementia are apparent clinically, it is relatively late in the disease process and neuronal destruction has already begun.3,7
Based upon this model, the earliest pathological event is the abnormal accumulation of forms of A-beta.6,7,8
Caption:
References
- Mayeux R and Stern Y. Epidemiology of Alzheimer Disease. In: Selkoe DJ, Mandelkow E, and Holtzman DM, ed. The Biology of Alzheimer Disease. New York: Cold Spring Harbor Laboratory Press; 2012:1-19.
- Alzheimer’s Disease Education & Referral (ADEAR) Center. Alzheimer's Disease: Fact Sheet. NIH Publication No. 11-6423 12 July 2021. Available at http://www.nia.nih.gov/alzheimers/publication/alzheimers-disease-fact-sheet. Accessed October 21, 2021.
- Serrano-Pozo A, Frosch MP, Masliah E, and Hyman BT. Neuropathological Alterations in Alzheimer Disease. In: Selkoe DJ, Mandelkow E, and Holtzman DM, ed. The Biology of Alzheimer Disease. New York: Cold Spring Harbor Laboratory Press; 2012:1-23.
- Aisen PS, Cummings J, Jack CR Jr, et al. On the path to 2025: understanding the Alzheimer's disease continuum. Alzheimers Res Ther. 2017;9(1):1-10.
- Blennow K, Zetterberg H, Fagan AM. Fluid Biomarkers in Alzheimer Disease. In: Selkoe DJ, Mandelkow E, and Holtzman DM, ed. The Biology of Alzheimer Disease. New York: Cold Spring Harbor Laboratory Press; 2012:1-23.
- Selkoe DJ and Hardy J. The amyloid hypothesis of Alzheimer's disease at 25 years. EMBO Mol Med (2016)8:595-608.
- Jack CR Jr, Knopman DS, Jagust WJ, Shaw LM, Aisen PS, Weiner MW, Petersen RC, Trojanowski JQ. (2010) Hypothetical model of dynamic biomarkers of the Alzheimer's pathological cascade. Lancet Neurology. 9(1):119-28.
- Selkoe DJ. (2011) Alzheimer Disease. Cold Spring Harbor Perspectives Biology. 3(7):1-17.
It’s time to intervene early to help make a difference for your patients2,3,7
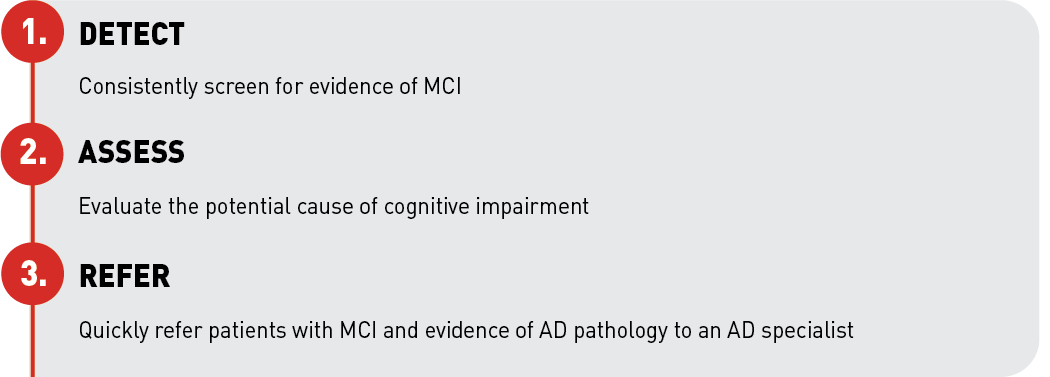
Image depicting steps for intervening early to help make a difference for patients: 1) Detect: Consistently screen for evidence of MCI. 2) Assess: Evaluate the potential cause of cognitive impairment. 3) Refer: Quickly refer patients with MCI and evidence of AD pathology to an AD specialist.
Commercially available blood-based biomarker tests used to detect amyloid positivity are not standalone tests. The results must be interpreted in conjunction with clinical assessment results. Patients must meet testing criteria.
Timely referral to an AD specialist can enable earlier consideration of disease-modifying therapies for patients who are in the early symptomatic stages of AD.2
Explore cognitive assessment in early‑stage AD
References:
- Aisen PS, Cummings J, Jack CR Jr, et al. On the path to 2025: understanding the Alzheimer’s disease continuum. Alzheimers Res Ther. 2017;9(1):60. doi:10.1186/s13195-017-0283-5
- Porsteinsson AP, Isaacson RS, Knox S, et al. Diagnosis of early Alzheimer’s disease: clinical practice in 2021. J Prev Alzheimers Dis. 2021;8:371-386. doi:10.14283/jpad.2021.23
- Sabbagh MN, Lue LF, Fayard D, et al. Increasing precision of clinical diagnosis of Alzheimer’s disease using a combined algorithm incorporating clinical and novel biomarker data. Neurol Ther. 2017;6(suppl 1):S83-S95. doi:10.1007/s40120-017-0069-5
- Alzheimer’s Association. 2025 Alzheimer’s disease facts and figures. Alzheimers Dement. Published online April 29, 2025. doi:10.1002/alz.70235
- Centers for Disease Control and Prevention. About Alzheimer’s. Updated August 15, 2024. Accessed September 22, 2025. https://www.cdc.gov/alzheimers-dementia/about/alzheimers.html
- Galvin JE, Aisen P, Langbaum JB, et al. Early stages of Alzheimer’s disease: evolving the care team for optimal patient management. Front Neurol. 2021;11:592302. doi:10.3389/fneur.2020.592302
- McDade E, Bednar MM, Brashear HR, et al. The pathway to secondary prevention of Alzheimer’s disease. Alzheimers Dement (N Y). 2020;6(1):e12069. doi:10.1002/trc2.12069
- Alzheimer’s Association. 2024 Alzheimer’s disease facts and figures. Alzheimers Dement. 2024;20(5):3708-3821. doi:10.1002/alz.13809
- Iwatsubo T, Irizarry MC, Lewcock JW, et al. Alzheimer’s targeted treatments: focus on amyloid and inflammation. J Neurosci. 2023;43(47):7894-7898. doi:10.1523/JNEUROSCI.1576-23.2023
- Jack CR Jr, Andrews JS, Beach TG, et al. Revised criteria for diagnosis and staging of Alzheimer’s disease: Alzheimer’s Association Workgroup. Alzheimers Dement. 2024;20(8):5143-5169. doi:10.1002/alz.13859
- Albert MS, DeKosky ST, Dickson D, et al. The diagnosis of mild cognitive impairment due to Alzheimer’s disease: recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimers Dement. 2011;7(3):270-279. doi:10.1016/j.jalz.2011.03.008
- National Institutes of Health, National Institute on Aging. What are the signs of Alzheimer’s disease? Accessed November 21, 2022. https://www.nia.nih.gov/health/what-are-signs-alzheimers-disease
- Potashman M, Buessing M, Levitchi Benea M, et al. Estimating progression rates across the spectrum of Alzheimer’s disease for amyloid-positive individuals using National Alzheimer’s Coordinating Center data. Neurol Ther. 2021;10(2):941-953. doi:10.1007/s40120-021-00272-1
- Data on File. Lilly USA, LLC. DOF-DN-US-0043.
- Mattsson-Carlgren N, Andersson E, Janelidze S, et al. Aβ deposition is associated with increases in soluble and phosphorylated tau that precede a positive Tau PET in Alzheimer’s disease. Sci Adv. 2020;6(16):eaaz2387. doi:10.1126/sciadv.aaz2387
- Selkoe DJ, Hardy J. The amyloid hypothesis of Alzheimer’s disease at 25 years. EMBO Mol Med. 2016;8(6):595-608. doi:10.15252/emmm.201606210
- Chen GF, Xu TH, Yan Y, et al. Amyloid beta: structure, biology and structure-based therapeutic development. Acta Pharmacol Sin. 2017;38(9):1205-1235. doi:10.1038/aps.2017.28
- Jack CR Jr, Bennett DA, Blennow K, et al. NIA-AA Research Framework: toward a biological definition of Alzheimer’s disease. Alzheimers Dement. 2018;14(4):535-562. doi:10.1016/j.jalz.2018.02.018